



Consider exploring topics from across the top or click the More button on the right choosing proteinuria, PKD health, PKD symptoms, Failing kidneys, PKD research, Transplants, Dialysis. Words in brown are links. This site contains details on cystic organ disease. If you cannot find what you are looking for, contact us, try the search engine or the language translator located at the bottom.

PKD
Polycystic Kidney Disease affects kidney tissue by changing the basic structure filling kidneys with multiples of cysts. Cystic cells replace normal functioning kidney tissue. The cystic kidney cells die and are not capable of being replaced. Eventually for some, polycystic kidneys can start a path toward decreased kidney functioning, eventually culminating with dialysis and/or organ transplant. However, polycystic Liver cells can regenerate new liver cysts. This regeneration produces an expansive liver. Both conditions are inherited, passed within families through the genes. By maintaining the integrity of ones own personal DNA, this can squelch the second hit mechanism that causes an increase in cyst numbers and symptoms.
You can change the health of your cystic organs. It is possible. Individuals with PKD normally have acidic urine. This contributes to elevations in uric acid. 24% of individuals with PKD have full blown gout. Acidic urine can raise uric acid. High uric acid can expand into gout symptoms. This all can contribute to kidney stone formation. By decreasing oxalates, purine foods, eating alkaline, lowering blood pressure, lowering proteinuria, eating less protein foods, eating less salt and drinking loads of water, all hopefully results in PKD Polycystic Kidney Disease kept under control. A very long genetic medical article explains much about PKD.
40% PKD'rs never require dialysis or transplant. Many of us are striving to be included with these healthy individuals. Among our personal choices, are which foods do we eat? Do we smoke? Do we exercise? Do we drink sufficient water? Some have been successful by adjusting these items.
We can modify our exposure to chemicals and kidney toxins. We can adjust how much exercise we do. We can self monitor and record blood pressure readings. We can maintain a running record of past blood pressure readings. We can decide how much water to drink. We can choose to eat foods low in salt. We can adjust our diet so we eat more alkaline plant based foods. We can find the means to lower our stress, enhance relaxation, and increase the blood flow to our kidneys.
With much guided attention from our personal physicians to these many details, we can exert some influence in maintaining health especially the health of polycystic kidneys. This can all begin to incline us toward the lucky 40% of PKD'rs who have healthy PKD polycystic kidneys throughout their lifetime.
We are unable to influence certain things in our lives. We cannot decide which gene we inherited: PKD2, or the more common PKD1 gene, a more aggressive form with an earlier onset of symptoms.
We have no control if we are born male or female. Males with PKD have a higher incidence of cardiac problems and proceed earlier to left ventricular heart failure. If we are born female, and have liver cysts, there is a increased chance of developing severe PLD Polycystic Liver Disease. In both instances these symptoms are hormone related. We can continue to take special care with our overall health. For it is generally our hearts not our kidneys that leads to our eventual demise.
For various reasons, sometimes family members hesitate to get tested for PKD with an MRI until they reach 30. ADPKD has been discovered as early as in utero. A screening test could be a combination of blood pressure checks and a check for protein in the urine. These are two early symptoms that can indicate some type of kidney disease. With a family history of PKD, it is likely to be PKD. These tests can often be found at health fares at a minimal cost.
How is ADPKD Passed Onto Children?
Each child of a parent with ADPKD has a 50% chance of inheriting the disease, because the gene for ADPKD is dominant. The prospects are similar to a flip of a coin. So, although 1 in every 2 children has a chance of inheriting ADPKD, sometimes both or neither will be affected. This form of inheritance is called Autosomal Dominant inheritance.
Definition of ADPKD
- At least 2 cysts in one kidney or a single cyst in each kidney (less than 30).
- At least 2 cysts in each kidney in individuals between 30-59.
- At least 4 cysts in each kidney in individuals 60 years or older.
There are two genes known to be associated with ADKPD. PKD1 is found in approximately 85 percent of individuals who have ADPKD. This is the more aggressive gene; diminished kidney functioning can occur in the 40's. PKD2 is found in about 15 percent of individuals who have ADPKD. Symptoms do not usually appear until the 60's.
Kidney Cysts Other Than PKD
Simple cysts of the kidney are known to occur and are of no known consequence. Parapelvic kidney cysts can also occur. Their development is followed by imaging. Renal cell carcinoma has been found in conjunction with PKD and can usually be spotted by imaging with an MRI.| Stage | Description | GFR |
| Stage 1 CKD | Slight kidney damage | > 90 |
| Stage 2 CKD | Mildly ↓ kidney function | 60-89 |
| Stage 3 CKD | Moderately ↓ kidney function | 30-59 |
| Stage 4 CKD | Severely ↓ kidney function | 15-29 |
| Stage 5 CKD | Kidney failure | < 15 (or dialysis) |
Some Useful Links
Food Analyzer
GFR Calculator
Kt/V Calculator
Kt/V is a tool used by nephrologists to determine the adequacy of dialysis treatment.
The DaVita Kt/V Calculator uses the Daugirdas II equation for Single Pool
(spKt/V), the Leypoldt equation for Equilibrated Double Pool (eKt/V) and
the Leypoldt equation for Standard (stdKt/V) calculations.
Hormones Kidneys Produce
Active form of vitamin D (calcitriol or 1,25 dihydroxy-vitamin D), which regulates absorption of calcium and phosphorus from foods, promoting formation of strong bone.
Erythropoietin (EPO), which stimulates the bone marrow to produce red blood cells.
Renin, which regulates blood volume and blood pressure.
Maintain kidney health early
- Eliminate Animal Proteins to ↓ Proteinuria
- Essential Amino Acids
- Use of essential amino acids from Calwood a formula designed for kidney patients. A newspaper article from Malaysian Times, Saving Failing Kidneys, explains how some countries are managing declining kidney functioning without the resources to pay for dialysis or organ transplants. A few PKD'rs have had limited success by working with their nephrologists and following the recommendations of Dr. Mackenzie Walser's book called Coping with Kidney Disease
- Albumin
- Phosphorus
- Potassium
- Coping with Kidney Disease
- EAA Essential Amino Acids
- Transplant
- Study suggests breakthrough in organ transplants
- Paired Organ - some have made use of the organ exchange program and plasmaphoresis.
- Dialysis - hemodialysis or peritoneal dialysis
When Kidney Functioning is Less than 30%
When Kidney Functioning is Less than 20%
-
Doctors begin dialysis preparations for patients when kidney functioning is less than
20%. They keep a careful watch with monthly blood work checks on kidney functioning levels, on
albumin levels; on potassium levels; on phosphorus levels; and base excess or alkalinity.
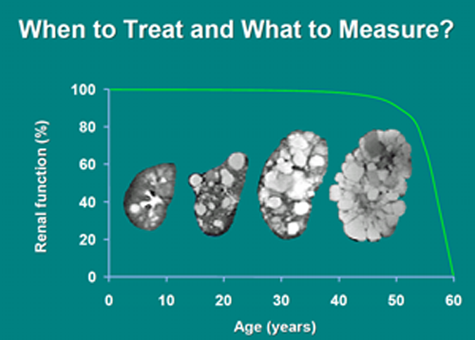
2015 Rationale for early treatment of polycystic kidney disease
From the above article:
"Renal injury begins with the formation of the first cyst. Counseling, regular exercise, limitation of dietary calories, salt,
protein and fat, increased fluid intake throughout the day and treatment of hypertension are components of a rational treatment
program that can be offered at an early age to those with, or at risk for developing PKD."
