From an interview with Dr. Brenner. - To open the link for Dr. Brenner's Bio, mouse over the words - Barry
Brenner, MD biography
HOW DOES PROTEIN STAY ON THE BLOOD SIDE OF THE GLOMERULUS AND NOT EMPTY INTO THE URINE?
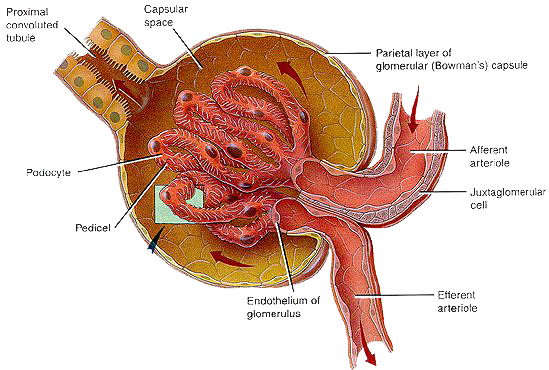
The glomerulus, enclosed in a capsule, Bowman’s capsule, is the main filter of the nephron. The nephron is the functioning unit of the kidney.
A tightly linked mesh of capillaries, make up the glomerulus of the kidney. Protein from the blood comes in contact with this linked mesh of capillaries. Studies show that these tightly linked mesh of capillaries, making up the glomerulus, is what keeps the proteins albumin and immunoglobulin in the blood, and out of the urine. In addition, both the walls of the capillaries and the proteins that circulate in the blood are both negatively charged; so they naturally repel and this also prevents protein from passing through the glomerulus into the urine. It is this naturally repelling charge that further protects proteins from passing into the urine coupled with a tightly knit mesh of glomeruli capillaries. No one had previously appreciated this charge-and-mesh property.
WHEN WE SEE HIGH PROTEIN LEVELS IN THE URINE, WHY HAS THIS TYPICALLY TIGHT BARRIER BROKEN DOWN?
Glomeruli have a charge-and-mesh property that is effected by an increase in pressure. Further studies demonstrated that, with proteinuria, the holes in the mesh get bigger and the negative charge disappeared. In the laboratory kidney disease was replicated by removing a kidney. This removes a large number of nephrons, which are made up of the filtering capillaries of the glomerulus and a tubular system essential for maintaining balance. Removing half of the nephrons causes the remaining nephrons to overwork, resulting in a progressively failing kidney. The more nephrons lost, the shorter the life span of the remaining kidney.
HOW DO WE SLOW DISEASE PROGRESSION?
Dr. Henry Christian, in 1913 prescribed low-protein diets. Lowering dietary protein enabled those with kidney disease to live longer. In the laboratory Dr. Barry Brenner discovered that increasing dietary protein increases glomerular pressure, and the glomerulus works best under a lower pressure. Animal proteins or an excess dietary proteins increases the kidney glomerular pressure. This increase in pressure causes circulating proteins to lose their negative charge and concurrently the linked mesh of capillaries that make up the glomerulus becomes bigger allowing more proteins to pass through to the urine from the circulating blood. Perhaps this can help explain how potassium citrate diminish proteinuria There have been clinical trials with potassium citrate concluding that it lowers pressure.
As far back as 1913 we have known that low protein diets enable individuals with kidney disease to live longer, many were unwilling to follow such a diet. Doctors tried lowering glomerular pressure through lowering blood pressure.
Luckily, Angiotensin Converting Enzyme Inhibitors (ACE Inhibitors) had just appeared. Kidney life was prolonged indefinitely by blocking the formation of Angiotensin II. It took 8 years from Dr. Brenner’s rat experiments to confirm these findings in humans, but today renal patients worldwide are treated with ACE inhibitors.
In 1957 the late Dr. Mackenzie Walser took this further. By combining ACE inhibitors, low protein diets (0.3 grams/kilogram of body weight), alkalinity, correcting anemia, supplementing with essential amino acids he has had success in halting end stage renal disease. If individuals only dropped the protein intake and took the essential amino acids [Calwood Amines], 30% of individuals were affected positively. If they took ACE inhibitors 40% of individuals were affected. But with the combination of both this figure jumped to 90% decrease in proteinuria. Dr. Walser discovered that serum albumin can be increased by eliminating dietary proteins and supplementing with essential amino acids, useful for many dialysis patients.
Dr. Mackenzie Walser's book Coping with Kidney Disease outlines a plan to try with your nephrologist:
• Eliminate all animal protein
• Reduce dietary protein 0.3 grams/kilogram of body if near end stage renal disease.
• Supplement with essential amino acids (specifically from Calwood)
• Lower blood pressure 110/70 - 120/80
• Maintain alkalinity with diet or alkalizer such as sodium citrate/potassium citrate
• Correct anemia
Scientists took urine samples of the entire population of the city of Groningen, Netherlands and found that among 80,000 tested, 3000 people were discovered to have protein in the urine. They identified a renal risk factor and are now working towards prevention. Their research has led to 39 papers published in 5 years on the impact of microscopic amounts of protein in the urine. Dialysis and transplantation in the United States this year alone will cost $25 billion. Governments in 80% of the world cannot afford dialysis or transplantation at all; for them kidney failure is fatal for most of their citizens.
Dr. Lin in China has a huge clinical trial from 17 centers testing ACE blood pressure medications or ARB (ACE receptor site blockers) along with low protein no animal protein diets. Preliminary results are very good.
From the latest water research, specifically for PKD'rs, one might consider adding to PKD Diet, drinking water; twice the amount of ones output.

 The hyperfiltration theory: A paradigm shift in nephrology or Gorge on Steak like a lion decrease kidney functioning.
The hyperfiltration theory: A paradigm shift in nephrology or Gorge on Steak like a lion decrease kidney functioning.
Remission
of renal disease: recounting the challenge, acquiring the goal
Overt proteinuria in PKD Established proteinuria and micro albuminuria in autosomal dominant polycystic kidney disease patients are associated with increased mean arterial pressure and more severe renal cystic involvement.
Reducing albuminuria
is a target for renoprotective therapy
Reducing
albuminuria a therapeutic target for cardiovascular protection with
nephropathy
Adult hypertension
and kidney disease: the role of fetal programming
Control of glomerular hypertension limits glomerular injury in rats.
Hyperfiltration
in remnant nephrons: a potentially adverse response to renal ablation. This article suggests
that controlling glomerular hypertension limits kidney injury in
the animal model. Renal ablation is accompanied by structural lesions and further
suggests that sustained single nephron hyperfiltration may have maladaptive consequences by damaging remnant glomeruli.
Written in 2001, Dr. Brenner commented that it took 8 years from the laboratory for this to be translated
into care options for humans with kidney disease.
Reduction
in albuminuria is associated with a proportional effect on renal protection. The above article has implications for using proteinuria levels for
testing future kidney protecterants.
Renal Protection in Patients Barry Brenner, MD 2002 Enroll in HDCN. Its free.
Angiotensin Receptor Blockers Optimal Reduction of Proteinuria Weiner MD 2000
Dialysis and transplantation in the United States this year alone will cost $25 billion. Governments in 80% of the world cannot afford dialysis or transplantation at all; for them kidney failure is fatal for most of their citizens. Dr. Lin in China has a huge clinical trial from 17 centers testing ACE blood pressure medications or ARB (ACE receptor site blockers) along with low protein no animal protein diets. Preliminary results are very good. The HALT Study is testing this with PKD.