PKD Clinical trials for water are beginning in New York City. For the PKD water clinical trial click here. In Tokyo, Japan doctors there are looking at water as a treatment for PKD. There is a second clinical trial involving water in Kansas City USA. Short excerpts taken from these interesting papers are written beside each article. For some interesting information on bottled water click here
 This star is a tiny droplet of water that was exposed to the word Truth, frozen, then photographed.. This is the water crystal that Truth forms. This star is a tiny droplet of water that was exposed to the word Truth, frozen, then photographed.. This is the water crystal that Truth forms.
From EWG:
Here is some information on city water supplies in the USA
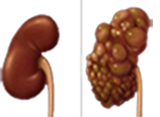
Water a possible treatment for PKD? Recently published PKD medical research
points to the possibility that by increasing water intake, we can slow
down kidney decline and cyst growth. In the PKD model, this has resulted
in a reduction in plasma vasopressin levels; renal cyst cell proliferation
decreased; and in the rats who increased their water intake, they slowed
PKD progression; diminished kidney cyst growth; and these PKD models
developed smaller cystic kidneys with a lower number of kidney cysts.
Sustained hydration might be beneficial to PKD’rs especially early
in the disease by limiting the detrimental effects of vasopressin. The
rats drank the equivalent of 20 liters of water per day. Human clinical
trials have yet to begin but are certainly warranted. This works in both
ADPKD and ARPKD. No one can give an answer as to how much water should
PKD’rs drink, but common sense says sufficient water intake would
be to keep plasma vasopressin levels near a point that renders urine
osmolality equal to or modestly lower than that of plasma. To know for
certain how much of the water cure is prudent therapy, a carefully
controlled clinical trial seems justified. Some of us have tried 3 liters/
day. Others have tried about 8 liters/day. We have yet to see if this
makes a difference.
It is not known if this helps liver cysts or kidney cysts, but we are willing to give it a try. Send an email. One suggestion was to calculate daily urine output – if it is 1500 cc, then drinking twice this amount or about 3000 cc of water might be sufficient to shut down vasopressin or to take urine osmolality equal to that of plasma.
Increased Water Intake
Decreases Progression Polycystic Kidney Disease PCK Rat
Wallace D 2006 J Am Soc Nephrol 17: 2220–2227,
2006. doi: 10.1681/ASN.2006030251
Arginine vasopressin (AVP) is an important
antidiuretic hormone that mediates its effect through the activation
of vasopressin V2 receptors (AVPV2R) and the subsequent stimulation of
adenylyl cyclase and synthesis of cAMP (10). . .Normally, urine is concentrated
to an osmolality that is greater than plasma. Day-to-day maintenance
of urine output depends on appropriate plasma AVP levels to regulate
osmotic water reabsorption by distal tubules and collecting ducts. Relatively
normal plasma levels of AVP may be sufficient to stimulate cyst epithelial
cell growth and renal enlargement in patients with PKD. Some patients
have an intrinsic defect in the capacity to concentrate urine maximally,
potentially leading to even greater levels of plasma AVP than normal
(11–13). . .Increased water intake sufficient to cause a reduction
in plasma (arginine vasopressin) AVP levels decreased renal cell proliferation,
and slowed PKD progression in PCK rats. We propose that sustained hydration
by increased water intake may be beneficial to some patients with PKD by
limiting the detrimental effects of (arginine vasopressin) AVP on renal cyst
growth.
Water for ADPKD? Probably, Yes
Torres V E 2006 Am Soc Nephrol 17: 2089–2091, 2006. doi: 10.168
1/ASN 2006060 60 3
Increased fluid intake may be beneficial
to some patients with ADPKD, at least in early stages of the disease, ,
, , If increased fluid intake, either by
itself or together with the administration of V2 receptor antagonists,
is proved to slow the rate of growth of polycystic kidneys, then its
long-term safety will need to be considered. . . .A number of studies of
other possible treatments for PKD have been published during 2005 to 2006.
Long-acting octreotide may inhibit cAMP production. . .Rapamycin, an inhibitor
of mammalian target of rapamycin (32–34), have been effective in
animal models of cystic disease. The pace of development of new potential
therapies for ADPKD raises the hope that its inexorable clinical course
soon may be modified. .Caffeinated beverages should be discouraged because
caffeine inhibits phosphodiesterase; enhances cAMP accumulation; and potentates
the effects of vasopressin on chloride secretion, cell proliferation, and
cyst growth, at least in vitro . . Calorically sweetened beverages and fruit
drinks are major contributors to the epidemic of obesity in the United
States and should be avoided (28). Because drinking tap water has been
associated in some studies with a slightly increased risk for bladder cancer
in men, whereas non-tap water has not, high-quality or bottled water may
be preferable . . .A retrospective analysis of the MDRD study (139 participants
with and 442 without ADPKD; GFR at entry 25 to 55 ml/min per 1.73 m2) was
performed to examine the relationship between fluid intake (reflected by
24-h urine volume and urine osmolality) and renal disease progression.
Higher urine volumes and lower urine osmolality is associated with
faster GFR decline regardless if the patient had ADPKD. The authors
considered two possible explanations. The first was that excessive fluid
intake and high urine volume cause faster renal disease progression and
possibly cyst growth in ADPKD. The second was that high urine volume with
low urine osmolality is the result and not the cause of faster renal disease
progression (19). The results by Nagao et al. (18) do not support the first
explanation; on the contrary, they suggest that increased fluid intake
may be beneficial to some patients with ADPKD, at least in early stages
of the disease. . .Long-acting octreotide may inhibit cAMP production,
and a pilot study of patients with ADPKD has shown promising results
(30). PD184352, an inhibitor of mitogen-activated protein kinase/ extracellular
signal–regulated kinase (31), and rapamycin, an inhibitor of mammalian
target of rapamycin (32–34), have been effective in animal models
of cystic disease. The pace of development of new potential therapies for
ADPKD raises the hope that its inexorable clinical course soon may be modified.
Vasopressin
Directly Regulates Cyst Growth in Polycystic Kidney
Torres V E 2008 Am Soc Nephrol. 2008 Jan;19(1):102-8. Epub 2007 Nov 21.
These observations indicate that AVP is a powerful modulator of cystogenesis
and provide further support for clinical trials of V2 receptor antagonists
in PKD.
Therapy for Polycystic
Kidney Disease? It’s
Water
Grantham JJ 2008 J Am Soc Nephrol 19: 1–2, 2008. doi: 10.1681/ASN.2007101100
Now we are confronted by the bizarre prospect that
water is the“cure” for
hereditary diseases that grotesquely bloat the kidneys with . . . water.
. .Cysts arise in renal tubules when epithelial cells
focally proliferate, leading to tiny outpouchings, that progressively
expand, upstream fluid from glomerular filtrate fills the budding cyst
cavity. Later, after they separate from the parent tubules. Two ordinarily
quiescent renal processes, epithelial cell proliferation and solute-driven
fluid secretion, come storming out of hiding and push a relatively small
number of cystic segments to take over eventually the parenchymal landscape,
driving functional glomeruli and tubules into oblivion. .We knew this
much about PKD for more than a decade. . .Although studies clearly implicate
a central role for vasopressin and cAMP in promoting kidney enlargement
and reducing renal function in PKD, a study from the Mayo laboratory
in this issue of the JASN9 provides definitive proof. The dramatic results
in this report are consonant with the view that epithelial cell growth
is of paramount importance to the formation of the cyst as well to the
overall increase of renal size in ARPKD. . .Of the hormones capable of
increasing cAMP production in collecting ducts, only AVP (arginine vasopressin)
is persistently elevated in the plasma of humans. Where do the cysts
form in ARPKD? In collecting ducts. Land based animals are normally antidiuretic
for most hours of the day and night, except for short periods when relatively
large volumes of water are imbibed. Therefore, plasma AVP levels are
usually high enough to activate adenylyl cyclase, generate cAMP, activate
aquaporin-2, increase collecting duct permeability to water, and concentrate
urinary osmolality above that of plasma. Thus, cyst growth is “clamped” by
vasopressin. . .How much water should I drink now? Patients
have already figured out that if extra water decreases vasopressin
and cAMP levels, then why isn’t plain old water a useful therapy?
No one can give an informed, definitive answer to that question, but
common sense leads me to think that sufficient water should be drunk
to keep plasma vasopressin levels near a point that renders urine osmolality
equal to or modestly lower than that of plasma. To know for certain
how much of the “water cure” is prudent therapy, a carefully
controlled clinical trial seems justified.
Sirolimus Reduces Polycystic Liver Volume in ADPKD Patients After Renal
Transplantation
Torres V E 2008 J Am Soc Nephrol. 2008 Mar;19(3):631-8. Epub 2008 Jan 16
Treatment with sirolimus was associated with decreased
polycystic liver volume, perhaps by preventing aberrant activation of
mTOR in epithelial cells lining the cysts.
Sirolimus ameliorates the enhanced expression of metalloproteinases in
a rat model of autosomal dominant polycystic kidney disease.
Berthier CC 2007 Nephrol Dial Transplant. 2008 Mar;23(3):880-9. Epub 2007
Nov 27.
Sirolimus treatment was associated with a marked improvement of MMP-2
and MMP-14 overexpression, and this
correlated also with less matrix and TBM alterations and milder cystic
disease.
Therapeutic intervention for autosomal dominant polycystic kidney disease.
Edelstein CL 2008 Nephrol News Issues. 2008 Mar; 22(3):25-6
Water Prescription for PKD
Clin J Am Soc Nephrol. 2011 Jan;6(1):192-7. Epub 2010 Sep 28.
Design, setting, participants, & measurements In eight ADPKD patients eating typical diets, osmolality and volume were measured in 24-hour urine collections. The amount of additional ingested water required daily to achieve a mean urine osmolality of 285 ± 45 mosm/kg was determined. Participants were instructed to distribute the prescribed water over waking hours for each of 5 days. Blood chemistries, 24-hour urine collections, BP, and weight were measured before and after the period of supplemental water intake. Results Five patients achieved the 285 mosm/kg urine target without difficulty. Mean urine osmolality decreased and mean urine volume increased; serum sodium, weight, and BP were unchanged. Daily osmolar excretion remained constant, indicating a stable ad lib dietary intake of solutes and protein over the 2-week study period. Conclusions The amount of additional water needed to achieve a urine osmolality target can be approximated from the urine osmolar excretion in ADPKD patients eating typical diets, providing a quantitative method to prescribe supplemental water for such individuals.
WATER
Here is some information on water from the EWG. The city water from Honolulu and Minneapolis tastes unusually sweet and delicious. Both cities are listed among the top ten (10) city water supplies. |