|
Surgical
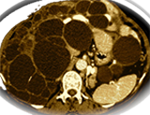
management of polycystic liver disease Massive hepatomegaly can lead to disabling symptoms of abdominal pain, early
satiety, persistent nausea, dyspnea, ascites, biliary obstruction, and lower
body edema. Earlier transplantation in appropriate candidates would seem to offer
a greater chance of improved outcomes, meaningful recovery, and return to their
prior functional status and quality of life. These patients had severe anorexia,
physical exhaustion, and evidence of malnutrition from end-stage PCLD for liver
transplant for APLD.
Polycystic liver disease: multimodality imaging
for complications and transplant evaluation. Cyst fenestration with partial hepatic resection and liver transplantation are
two therapies that provide more permanent resolution of symptoms in patients
with extensive hepatic involvement. Help the radiologist provide the referring
clinician with important information for therapeutic decision making. RSNA, 2006.
Liver and kidney transplantation for polycystic
liver and kidney-renal function and outcome. Transplantation is an excellent option for PLD with dramatic improvement in quality
of life and acceptable morbidity. acceptable renal function at time of transplantation,
solitary liver transplantation has an excellent outcome.
Liver transplantation in polycystic liver disease:
A relevant treatment modality for adults? We conclude that patients treated for PLD by LTX have a good long-term prognosis
and excellent relief of symptoms and that LTX might be considered in severe cases
of PLD, where conventional surgery is not an option.
Results of percutaneous sclerotherapy and surgical
treatment in patients with symptomatic simple liver cysts and polycystic liver
disease. Results of percutaneous sclerotherapy and surgical treatment for PLD are disappointing.
Outcome and Quality of Life in Patients With
Polycystic Liver Disease After Liver or Combined Liver-Kidney Transplantation. Patients with advanced polycystic liver or polycystic liver-kidney disease have
an excellent survival rate and an improved quality of life after liver or combined
liver-kidney transplantation.
New advances in evaluation and management of
patients with polycystic liver disease. In these patients, medical management alone has proved ineffectual. Therefore,
in the symptomatic APLD patient, surgical therapy remains the mainstay of therapy
and includes cyst aspiration and sclerosis, fenestration with and without hepatic
resection and orthotopic liver transplantation.
Successful transplantation of cadaveric polycystic
liver: case report and review of the literature. We report the successful
use of a polycystic donor liver and review the experience with this donor population.
We propose that the selective use of polycystic donor livers containing small
(less than 5 cm) cysts with preserved liver parenchyma is safe and appropriate.
Quality of Life and Liver Transplantation in
Patients With Polycystic Liver Disease. Chronic and end-stage liver diseases negatively affect many aspects of patients’ physical
functioning and quality of life. A considerable amount of research in the past
few decades has been devoted to the measurement of HRQL. Global (generic) aspects
of health-related quality of life are commonly assessed, which allows for comparisons
between patients with different diseases
|
|
Combined liver-kidney transplantation: indications and results
Ferhi K, Lakehal M, Avakian R, Bensallah K, Boudjema K, Patard JJ, Guille F.
Prog Urol. 2008 Apr;18(4):245-50. Epub 2008 May 8. French
Choice of transplantation techniques and indications for liver transplantation in polycystic liver disease in patients with no signs of end-stage liver disease.
Kornasiewicz O, Dudek K, Bugajski M, Najnigier B, Krawczyk M.
Transplant Proc. 2008 Jun;40(5):1536-8.
Sirolimus reduces polycystic liver volume in ADPKD patients.
Qian Q, Du H, King BF, Kumar S, Dean PG, Cosio FG, Torres VE.
J Am Soc Nephrol. 2008 Mar;19(3):631-8. Epub 2008 Jan 16.
ScienceDaily (Oct. 4, 2007) — Patients who undergo liver transplantation at age 60 or above experience fewer episodes of rejection.
Researchers, led by Timothy Cross of King's College Hospital in London, set out to retrospectively examine the transplant outcomes of older patients compared to younger ones. They included 416 patients transplanted at King's College between 1988 and 2003, dividing them into three groups according to age: Group 1 included 77 patients over age 65. Group 2 included 137 patients between 60 and 64 years old. And group 3 included 202 patients 18-59 years old. Each patient was regularly examined post-transplant for signs of rejection. Here is some good news for us oldsters. It seems likely we will have fewer episodes of rejection. I remember listening to a lecture by Dr. Robert Montgomery from Johns Hopkins University who began the first donor exchange living donor kidney transplant programs, wiith liver transplants organ rejection is not usually an issue.
Using two donors for a living donor liver transplant:
Living donor liver transplantation (LDLT) between adults inevitably implies two potential risks associated with a small-for-size graft for the recipient and small remnant liver for the donor. To overcome these problems, LDLT using dual grafts from two independent donors can be a solution, in which sufficient graft volume can be obtained while preserving donor safety. We present a case of LDLT that was managed successfully by using right and left lobe dual grafts from two donors. I met a lady two (2) years in a row at a PKD conference. She had massive severe PLD polycystic liver disease. In the interim between our first and second visit, she had obtained a double transplant of a kidney and liver, both from living donors. I was amazed at how good she looked, after receiving double transplants.
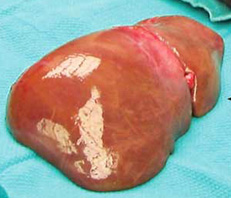 
NORMAL LIVER MASSIVE POLYCYSTIC LIVER PLD |